
| Admissions | Accreditation | Booksellers | Catalog | Colleges | Contact Us | Continents/States/Districts | Contracts | Distance Education | Emergency | Examinations | Forms | Grants | Hostels | Honorary Doctorate degree | Investment | Instructors | Lecture | Librarians | Membership | Professional Examinations | Programs | Progress Report | Recommendations | Research Grants | Researchers | Students login | School | Search | Seminar | Study Center/Centre | Sponsorship | Tutoring | Thesis | Universities | Work counseling |
Airway Anatomy
|
|
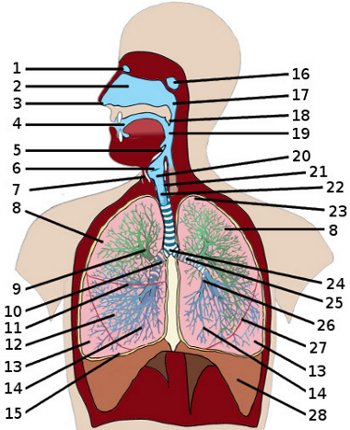
the respiratory system Question 1 : Normal resting respirations are ... 10 to 18 breaths per minute 60 to 80 breaths per minute 5 to 10 breaths per minute 10 to 18 breaths per minute Question 2 : Gas exchange in the lungs takes place in the ... trachea pleura alveoli alveoli Question 3 : Which number indicates the uvula? 18 20 5 18 Question 4 : Number 19 is pointing to the ... larynx oropharynx trachea oropharynx Question 5 : Which number indicates the sphenoid sinus? 1 2 16 16 Question 6 : Number 17 is pointing to the ... nasopharynx larynx oral cavity nasopharynx Question 7 : Which number indicates the larynx? 22 20 2 20 Question 8 : Number 21 is pointing to the ... carina epiglotis cricoid cartilage cricoid cartilage Question 9 : Number 27 is pointing to the ... horizontal fissure pleura oblique fissure oblique fissure Question 10 : The diaphragm is indicated by number ... 14 18 28 28 Question 11 : Which number indicates the trachea? 19 7 22 22 Question 12 : Number 23 is pointing to the ... apex pleura left primary bronchus apex Question 13 : The carina is indicated by number ... 24 23 7 24 Question 14 : Number 25 is pointing to the ... left secondary bronchus left primary bronchus right primary bronchus left primary bronchus Question 15 : The left secondary bronchus is indicated by number ... 9 26 25 26 |
Techniques for opening the airway
|
Basic airway management starts with assessment of the airway. Is the airway free of obstructions? Is the respiratory rate and volume adequate? It's a common belief that airway obstruction is usually caused by the tongue, yet studies have shown that the epiglottis and other soft structures in the hypopharynx are more likely responsible for these obstructions1. Suctioning and anatomical positioning such as the head tilt, chin lift or jaw thrust will in most circumstances relieve these obstructions regardless of the anatomy responsible for causing them. Oral airway devices: Oropharyngeal airways will relieve soft tissue obstruction of the posterior airway by displacement of the tongue and soft tissue anteriorly. They should only be used in the unconscious patient as vomiting, aspiration and laryngospasm may otherwise occur. There are two primary insertion techniques: 1.The airway device may be inserted sideways or upside-down and, once it is well into the mouth, rotated and advanced in to the full position 2.A tongue blade can hold the tongue in a down and forward position until the airway is in place Choose the method that works best for you so long as the end result is correct2. The desirable results: The patient is not responding with a gag reflex or snoring, and air is going in and out. Be vigilant in observing for vomiting. Nasal airway: The nasopharyngeal airway is another option. These are placed in either nasal passage and allow unobstructed routes for ventilation through the nose to the hypopharyngeal area. They tend to be less stimulating than the oral airway but can cause epistaxis. The base of the nasal passage is relatively flat and parallel to the roof of the mouth. When inserting the airway, lift slightly on the tip of the nose with the free hand, and place the lubricated airway straight into the passage with the bevel against the nasal septum, not upward as is the natural tendency. This limits contact with the turbinates and hopefully avoids the resultant nosebleed. The airway should be constructed of a soft, flexible material, and apply a water-based lubricant such as KY jelly prior to insertion2. Ventilation: Ventilating the patient after a clear airway has been established is the next technique to master. The American Heart Association's opinion on bag-mask ventilation is that when possible, it should be a two-person job. One provider should hold the mask with both hands and maintain proper position of the head while maintaining a good mask seal; the second provider should squeeze the bag. Because assigning two people for this task is not always practical, we should use good technique and do the best possible job for the given situation3. The bag-valve mask unit (BVM) should consist of a self-inflating bag, oxygen reservoir and non-rebreathing exhalation valve (NRV). The mask and NRV should be constructed of a clear see-through material to allow observation for emesis. The bag should have the ability to deliver 800 ml while squeezing with one hand. It should not require oxygen flow or volume in the reservoir to inflate, and it must be constructed of a non-slip material for easy grasp and be able to deliver an FiO2 of 0.85 to 1.04. First, choose the proper size mask for an optimal fit. The best fit is the smallest mask that will provide a good seal around the mouth and nose. This will cause the least amount of dead space and be easier to hold. For patients with thick beards, the edentulous or anyone with facial deformity from trauma, it will be difficult to maintain a good seal. Second, the mask should not be pressed down onto the face. This pressure will cause airway misalignment. The provider should for a "C" shape on the mask with the thumb and index finger and grasp the mandible with the remaining three fingers, pulling the face into the mask. This works best when using two hands but with practice can be accomplished with one. It will be easier for the provider to maintain correct positioning of the airway without the misaligning forces caused by pushing the mask down on the unsupported head and face. Third, ventilations should be delivered with emphasis on a slow inspiratory phase (1.5 to 2.0 seconds) in the non-intubated patient. This should keep airway pressures low and minimize gastric inflation. The target is a high volume-low pressure ventilation5. Advanced airway management will provide the best protection from aspiration. It is the most precise method for of control of the gases of respiration and supplies a medication route. However, the best advanced skills are of little value if the patient suffers a hypoxic insult during the basic airway management phase. Practice of high-quality basic skills is the foundation of good medical care. Advancing Airway Management: Opening and Maintaining the Airway 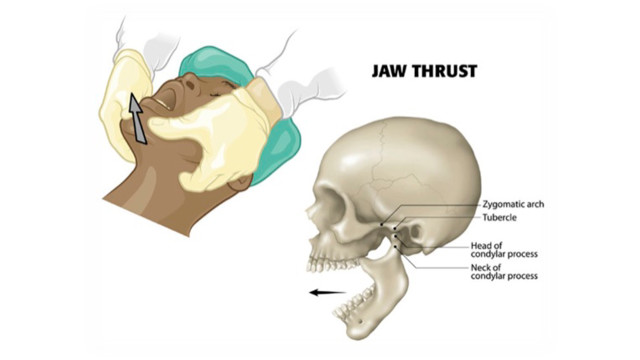 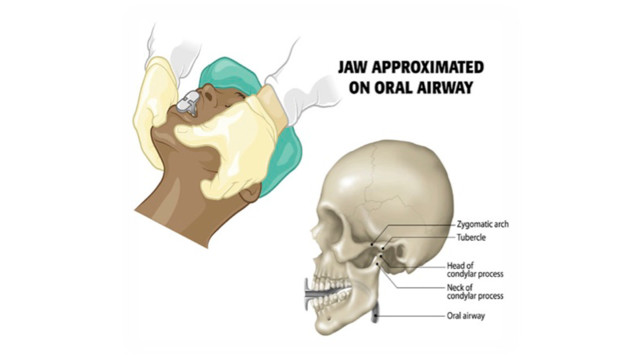 Advancing Airway Management: Laryngoscopy Here are further guidelines. |