
|
What Is a Normal Heart Rhythm? The heart has four chambers, or areas. During each heartbeat, the two uppers chambers (atria) contract, followed by the two lower chambers (ventricles). This action is directed by the heart's electrical system. The electrical impulse begins in an area called the sinus node, located in the upper part of the right atrium. When the sinus node fires, an impulse of electrical activity spreads through the right and left atria, causing them to contract, forcing blood into the ventricles. Then the electrical impulses travel in an orderly manner to another area called the atrioventricular (AV) node and HIS-Purkinje network. The AV node is the electrical bridge that allows the impulse to go from the atria to the ventricles. The HIS-Purkinje network carries the impulses throughout the ventricles. The impulse then travels through the walls of the ventricles, causing them to contract. This forces blood out of the heart to the lungs and the body. The pulmonary veins empty oxygenated blood from the lungs to the left atrium. A normal heart beats in a constant rhythm -- about 60 to 100 times per minute at rest. Normal Sinus Rhythm (NSR) In a normal heart rhythm, the sinus node generates an electrical impulse which travels through the right and left atrial muscles producing electrical changes which is represented on the electrocardiogram (ECG) by the p-wave. The electrical impulse then continue to travel through specialized tissue known as the atrioventricular node, which conducts electricity at a slower pace. This will create a pause (PR interval) before the ventricles are stimulated. This pause is helpful since it allows blood to be emptied into the ventricles from the atria prior to ventricular contraction to propel blood out into the body. The ventricular contraction is represented electrically on the ECG by the QRS complex of waves. This is followed by the T-wave which represents the electrical changes in the ventricles as they are relaxing. The cardiac cycle after a short pause repeats itself, and so on. 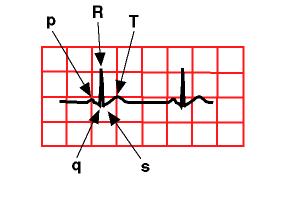
Therefore, on an ECG in normal sinus rhythm p-waves are followed after a brief pause by a QRS complex, then a T-wave. Normal sinus rhythm not only indicate that the rhythm is normally generated by the sinus node and traveling in a normal fashion in the heart, but also that the heart rate, i.e. the rate at which the sinus node is generating impulses is within normal limits. There is no one normal heart rate, but this varies by age. It is normal for a newborn to have a heart rate up to 150 beats per minute, while a child of five years of age may have a heart rate of 100 beats per minute. The adult's heart rate is even slower at about 60-80 beats per minute. Fast Heart Rate (Tachycardia) Sinus tachycardia: a fast heart rate may occur with a normal heart rhythm, this is called sinus tachycardia. This means that the impulse generating the heart beats are normal, but they are occurring at a faster pace than normal. This is termed sinus tachycardia and is seen normally with exercise or with excitement.  Supraventricular tachycardia (SVT). In this abnormal heart rhythm the impulse stimulating the heart is not generated by the sinus node, but instead comes from a collection of tissue around and involving the atrioventricular (AV) node. These electrical impulses from this abnormal site are generated at a rapid impulse, which may reach 280 beats per minute.  Atrial flutter: In this abnormal rapid heart rhythm the abnormal tissue generating the rapid heart rate is also in the atria, however, the atrioventricular node is not involved. Since the atrioventricular node is slow conduction tissue and it is not involved in this type of abnormal heart rhythm the heart rate in this case (atrial flutter) would be faster than that in supraventricular tachycardia where the atrioventricular node is involved in generating the abnormal heart rhythm and will cause it to be slower.  Ventricular tachycardia: This is a dangerous type of rapid heart rhythm because it is usually associated with poor cardiac output (amount of blood ejected out of the heart). It results from abnormal tissues in the ventricles generating a rapid and irregular heart rhythm. Slow Heart Rate Sinus bradycardia: The heart may slow down, yet maintain the normal pattern of rhythm (sinus), this is known as sinus bradycardia. It usually is benign and may be caused by medications such as beta blockers.  Atrioventricular block (AVB): the sinus node may be generating heart beats causing the atria to contract at a normal rate, however not every electrical impulse coming from the atria is being passed down to the ventricles by the atrioventricular node due to a block in conduction. There are various types of AV block depending upon the mechanism of block. Second degree AV block is when the impulse from the atria is blocked every certain number of beats.  While in complete AV block non of the atrial impulses pass through the atrioventricular node and the ventricles generate their own rhythm. Irregular Heart Rhythm Premature atrial contraction (PAC): The atria fires an early impulse which causes the heart to beat earlier causing irregularity in the heart rhythm.  Premature ventricular contraction (PVC): The ventricles fire an early impulse which causes the heart to beat earlier causing irregularity in the heart rhythm.  Atrial fibrillation: this is a result of many sites within the atria firing electrical impulses in an irregular fashion causing irregular heart rhythm. This type of abnormal heart rhythm is unusual in children.  |
|
1. What controls the normal rhythm of the heart? 2. How do autonomic nerves, circulating catecholamines, extracellular potassium concentrations, thyroid hormone, and hypoxia alter pacemaker activity? 3. How do autonomic nerves, circulating catecholamines, cellular hypoxia, and drugs blocking sodium channels alter conduction velocity within the heart? 4. What are arrhythmias? 5. Define each of the following types of arrhythmias: 1. sinus rhythm 2. sinus bradycardia 3. sinus tachycardia 4. sick sinus syndrome 5. atrial tachycardia 6. atrial flutter 7. atrial fibrillation 8. junctional escape rhythm 9. AV nodal blocks - first, second and third degree 10. supraventricular tachycardia 11. ventricular premature beat 12. ventricular tachycardia 13. ventricular flutter 14. ventricular fibrillation 6. How can altered automaticity and conduction cause arrhythmias? 7. What are early- and delayed-afterdepolarizations and what can cause them? 8. What are ectopic foci? 9. Under what conditions and by what mechanisms can a non-pacemaker cell become a pacemaker cell? 10. What are reentry currents, how can they lead to tachyarrhythmias, and how can changes in conduction velocity and the relative refractory period either precipitate or abolish reentry currents? 11. What are the hemodynamic consequences of arrhythmias? 1. What are the normal concentrations of sodium, potassium, and calcium ions inside and outside of a cardiac myocyte? 2. What is the Nernst potential? What is an equilibrium potential? 3. How does changing the concentrations of sodium, potassium, and calcium ions inside and outside the cell affect the resting membrane potential in cardiac cells? 4. What is the role of the sarcolemmal Na+/K+-ATPase in the generation and maintenance of cardiac membrane potentials? 5. How are calcium gradients maintained across the cardiac cell membrane? 6. How do changes in the relative ionic conductances of sodium, potassium, and calcium ions affect the membrane potential? 7. How are cardiac action potentials different from those found in nerve cells? 8. What ionic currents are responsible for pacemaker action potentials? 9. How do autonomic nerves, circulating catecholamines, extracellular potassium concentrations, thyroid hormone, and hypoxia alter pacemaker activity? 10. What ionic currents are responsible for non-pacemaker action potentials? 11. What is the effective refractory period (ERP) for an action potential and what can cause it to lengthen or shorten? 12. What is the normal sequence and pathways for depolarization within the heart? 13. How do autonomic nerves, circulating catecholamines, cellular hypoxia, and drugs blocking sodium channels alter conduction velocity within the heart? http://www.cvphysiology.com/Tutorials/Tutorial%20-%20normal%20and%20abnormal%20rhythms.htm |