How have surgical emergencies been categorized?
Pediatric surgical emergencies.
Adult surgical emergencies, age 19 and older.
What are examples with diagnosis of surgical emergencies?
There are more than 226 such examples of surgical emergencies.
General surgery emergencies
-
Abscesses
-
Appendicitis
-
Acute Pancreatitis
-
Acute mesenteric ischemia
-
Acute abdominal conditions
-
Amebic liver abscess
-
Biliary Colic & Cholecystitis
-
Bleeding from esophageal varices
-
Cholecystitis (gallbladder infection)
-
Complications of peptic ulcer, including perforated ulcer and bleeding ulcer
-
Diverticulitis
-
Gall bladder and bile duct disease
-
Intestinal volvulus
-
Incarcerated hernia
-
Incarcerated and Strangulated Inguinal Hernias
-
Intestinal obstruction
-
Massive Upper GI Haemorrhage
-
Peritonitis
-
Perforated Abdominal Viscus
-
Pelvic infections with abscesses
-
Perforated typhoid ulcers
-
Ruptured intestine
-
Rectal Bleeding
-
Stercoral perforation
-
Small Bowel Obstruction
-
Spleen Removal
-
Thrombosed hemorrhoids
Thoracic surgery emergencies
-
Acute airway obstruction/Airway obstruction
-
Tension pneumothorax
-
Massive haemothorax
-
Pneumothorax
-
Open pneumothorax
-
Flail chest segment with pulmonary contusion
-
Cardiac tamponade.
Colon and rectal surgery emergencies
-
Injury to the Colon and Rectum (stab wound)
-
Hemorrhoids
-
Fissures (painful tears in the anal lining)
-
Abscesses and fistulaes (infections located around the anus and rectum).
-
Hemorrhage of rectum and anus
Obstetrics emergencies
-
Abortion With Hemorrhagic Shock
-
Acute Abdominal Pain During Pregnancy
-
Amniotic Fluid Embolism
-
Antepartum Hemorrhage Placenta previa/accreta/percreta Placental abruption/Uterine rupture
-
Bleeding ectopic pregnancy
-
Chorioamnionitis
-
Cesarean Section Under Local Anesthesia
-
Cesarean Section Without Anesthesia
-
Cardiopulmonary Resuscitation During Pregnancy
-
Cesarean delivery: elective/Placenta Previa (if stable) or urgent (if hemorrhaging)
-
Disseminated Intravascular Coagulation
-
Eclampsia
-
Ectopic Pregnancy with Shock
-
Intrauterine fetal demise
-
Multiple gestation
-
Placenta accreta / placenta percreta
-
Placental abruption
-
Placenta previa
-
Preeclampsia/eclampsia
-
Premature Rupture of Membranes
-
Preterm Labor and Delivery
-
Prolapsed Umbilical Cord
-
Postpartum Hemorrhage Uterine inversion/Uterine atony/Genital tract trauma
-
Postmortem Cesarean Section
-
Retained Placenta
-
Retained abortion
-
Severe Preeclampsia
-
Shoulder Dystocia
-
Surgical complications in pregnancy (appendicitis, cholecystitis, major abdominal trauma, bowel obstruction, intracranial hemorrhage, adnexal mass, etc)
-
Trauma During Pregnancy
-
Uterine Rupture
-
Uterine Inversion
Gynecologic surgery emergencies
-
Adnexal torsion
-
Tubo-ovarian abscess, hemorrhagic ovarian cysts
-
Gynecologic hemorrhage
-
Vulvovaginal trauma.
Neurological surgery emergencies
-
Acute subdural hematoma
-
Subarachnoid hemorrhage
-
Intracranial Hemorrhage
-
Brain AVM (arteriovenous malformation)
-
Spine Fracture
-
CaudaEquina
-
Penetrating Injury
-
Intracranial Lesions –Focal
-
Open Skull fracture
-
Head Trauma
-
Cushing response
-
Epidural Hematomas
-
Epidural Hemorrhage
-
Uncal Herniation
-
Pituitary Adenoma
-
Pituitary apoplexy
-
Traumatic Compression Fracture
-
Jumped facets
-
Ballistic trauma or gunshot wound (GSW)
-
Shunt malfunction
-
T7-8 corptectomyand T6-T9 fusion
-
Cord compression
-
Clinical signs of high ICP
Ophthalmic surgery emergencies
-
Orbital Compartment Syndrome
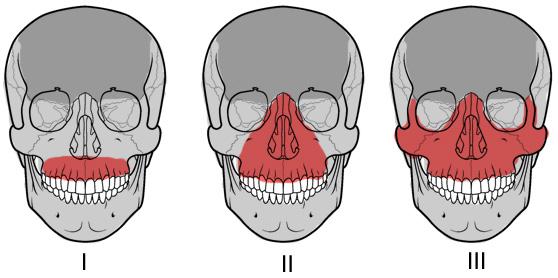
Oral and maxillofacial surgery emergencies
-
Dental extractions, including wisdom teeth
-
Dental implants and bone grafting
-
TMJ evaluations and management
-
Corrective jaw surgery
-
Facial infection treatment
-
Treatment of facial trauma
-
General oral surgery
-
Cosmetherapy, including botox, juvederm, and restylane
Orthopaedic surgery emergencies
Pediatric patients
Fractures.
-
Supracondylar humeral, femoral, and tibial conditions (such as slipped capital femoral epiphysis)
-
Septic arthritis
-
Limb- and life-threatening pathologies, including compartment syndrome
-
Dysvascular limb
-
Cervical spine trauma
-
Polytraumatized child
Patients ages 19 or more
Fractures.
-
Open fractures (bone is exposed outside of a wound)
-
Open fractures or joints
-
Fractures with joint involvement
-
Isolated breaks
-
Stress fractures
-
Multiple fractures
-
Non-union fractures (fractures that do not heal)
-
Malunion fractures (fractures that heal incorrectly)
-
Acute compartment syndrome
-
Neurovascular injuries
-
Joint dislocations
-
Ligament sprains
-
Muscle strains
-
Tendon injuries
-
Septic joints
-
Cauda equina syndrome
Otolaryngology emergencies
-
Epistaxis
-
Peritonsillar abscess
-
Retropharyngeal abscess
-
Acute external otitis
-
Auricular hematoma
-
Mastoiditis
-
Facial nerve paralysis/Bell’s palsy
-
Ramsey-Hunt syndrome
-
Nasal fracture
-
Septal hematoma
-
Orbital blow-out fracture
-
Sudden sensorineural hearing loss (SSNHL)
-
The red herring tonsil
-
Dental abscess
-
Facial cellulitis
-
Ludwig’s angina
-
Deep neck space infections
-
Angioedema
-
Sinusitis: complications
Pediatric surgery emergencies
-
Appendicitis
-
Intussusception
-
Pyloric Stenosis
-
Necrotizing Enterocolitis
-
Testicular Torsion
-
Incarcerated Inguinal hernia
-
Hirschsprung’s Enterocolitis
-
Incarcerated Hernia
-
Inguinal Hernia
-
Incarcerated Inguinal Hernia
-
Small Bowel Obstruction
-
NEC Pneumoperitoneum
-
Malrotation with volvulus
-
Bowel Obstruction
Atresias
Hirschsprung’s
Malrotation
Volvulus
Intussusception
-
Jejunal Atresia
-
NEC
-
The Acute Groin
-
Bleeding Meckel’s
-
Toxic Megacolon
-
Foreign Bodies
-
Esophageal Foreign Bodies
-
Bronchial Foreign Body
-
Imperforate Anus: Anal atresia
-
Anesthetic implications
Plastic and maxillofacial surgery emergencies
-
Burn Care
-
Bite Wounds
-
Burns and Frostbite
-
Cleft lip and palate repair
-
Compartment Syndrome
-
Examination of Hand Injuries
-
Facial Lacerations
-
Frontal Sinus Fractures
-
Frontal Sinus Fractures
-
Hand and Forearm Tendon Injuries
-
Hand and Wrist Fractures and Dislocations
-
Hand Infections and Injection Injuries
-
Hand Injuries
-
Ischemic Limb / Amputated Part
-
Laceration repair
-
Major Burn
-
Mandibular Fractures
-
Maxillofacial injuries
-
Nasal and Nasal-Orbital-Ethmoid (NOE) Fractures
-
Necrotizing Fasciitis
-
Orbit and Zygoma Fractures
-
Pressure Sores
-
Septic Joint
-
Suppurative Flexor Tenosynovitis
-
The Traumatized Face
-
Wound Management
Urology emergencies
Traumatic
-
Renal Trauma
-
Ureteral injury
-
Bladder Trauma
-
Urethral injury
-
Testicular Trauma
-
Genital Trauma
-
Penile trauma
Non traumatic
-
Acute Urinary Retention
-
Acute Scrotum Epididymo-orchitis/Testicular Torsion
-
Hematuria
-
Priapism
-
Paraphimosis
-
Renal Colic
-
Testicular torsion
-
Urinary Retention
-
Fournier's Gangrene
Vascular Surgery Emergencies
Vascular Emergencies
(not aneurysms)
Arterial
-
Acute ischaemia
-
Bleeding due to trauma (incl. iatrogenic)
Venous
-
Deep Venous Thrombosis (Phlegmesia Caeurlia Dolens)
-
Pulmonary Embolism
Lymphatic
-
Cellulititis
-
Compartment Syndrome
-
Occlusive Peripheral Vascular Disease
Peripheral vascular disease
-
Includes any disease affecting the peripheral vascular system
-
Occlusive – essentially blocked arteries
Ruptured aortic aneurysm
-
Aortic dissection
-
Internal bleeding
-
Limb ischemia
|
Types of surgical emergencies.
What should physician surgeon medical emergency know?
You have to know everything of these entities.
General surgery emergencies
Acute Abdomen
1.Assess urgency
2.How sick is the patient?
3.Take a history
4.Examine the patient
5.Urineanalysis
6.BhCG
7.Formulate differential diagnosis
8.Investigations
9.Decide to discharge, admit, observe, operate
Stratification of the Acute Abdomen
1.Pain only
2.Pain + systemic symptoms
3.Peritonitis -systemic symptoms
4.Localised peritonitis + systemic symptoms
5.Generalised peritonitis -systemic symptoms
6.Generalised peritonitis +systemic symptoms
Peritonitis and Intra-abdominal sepsis
•Inflammation of the serosal membrane
•Constellation of signs and symptoms; abdominal pain, muscle wall rigidity, systemic signs of inflammation
•Classification
1.Primary
2.Secondary
3.Tertiary
•Generalised vs localised
•Cause
Causes of Peritonism
| |
Upper GI |
HPB |
Small& Large Bowel |
GU |
| Infection / Inflammation |
Gastritis |
Cholecystitis
Pancreatitis
|
Gastroenteritis
Meckel's diverticulitis
Appendicitis
TB
IBD
Diverticulitis
|
PID
UTI
Obstructive Uropathy
|
| Perforation
|
Boerhaave syndrome
Peptic ulcer
Malignancy
Trauma
Iatrogenic
|
Gallbladder
Malignancy
Trauma
Iatrogenic
|
Diverticular
Stercoral
Ischaemia
IBD (Toxic megacolon)
Tumour
|
Ruptured ovarian cyst
Trauma
Iatrogenic
|
| Ischaemia
|
|
|
Mesenteric
Hernia
Close loop obstruction
|
|
Localised Peritonitis
•Bloods X-rays
•Establish differential diagnosis
•Initiate resucitation and management
•Watch, wait, act
|
What is emergency general surgery?
Appendicitis
Peritonitis
Evaluation of Acute Abdominal Pain in Adults
Acute abdomen
The term acute abdomen refers to a sudden, severe abdominal pain of unclear etiology that is less than 24 hours in duration. It is in many cases a medical emergency, requiring urgent and specific diagnosis. Several causes need surgical treatment.
Causes
The differential diagnoses of acute abdomen include but are not limited to:
1.Acute appendicitis
2.Acute peptic ulcer and its complications
3.Acute cholecystitis
4.Acute pancreatitis
5.Acute intestinal ischemia (see section below)
6.Diabetic ketoacidosis
7.Acute diverticulitis
8.Ectopic pregnancy with tubal rupture
9.Ovarian torsion
10.Acute peritonitis (including hollow viscus perforation)
11.Acute ureteric colic
12.Bowel volvulus
13.Acute pyelonephritis
14.Adrenal crisis
15.Biliary colic
16.Abdominal aortic aneurysm
17.Hemoperitoneum
18.Ruptured spleen
19.Kidney stone
20.Sickle cell anaemia
Ischemic acute abdomen
Acute abdominal pain can represent a spectrum of conditions from benign and self-limited disease to surgical emergencies. Evaluating abdominal pain requires an approach that relies on the likelihood of disease, patient history, physical examination, laboratory tests, and imaging studies. The location of pain is a useful starting point and will guide further evaluation. For example, right lower quadrant pain strongly suggests appendicitis. Certain elements of the history and physical examination are helpful (e.g., constipation and abdominal distension strongly suggest bowel obstruction), whereas others are of little value (e.g., anorexia has little predictive value for appendicitis).
Ultrasonography is recommended to assess right upper quadrant pain, and computed tomography is recommended for right and left lower quadrant pain. It is also important to consider special populations such as women, who are at risk of genitourinary disease, which may cause abdominal pain; and the elderly, who may present with atypical symptoms of a disease.
Abdominal pain is a common presentation in the outpatient setting and is challenging to diagnose. Abdominal pain is the presenting complaint in 1.5 percent of office-based visits1 and in 5 percent of emergency department visits.2 Although most abdominal pain is benign, as many as 10 percent of patients in the emergency department setting and a lesser percentage in the outpatient setting have a severe or life-threatening cause or require surgery.2 Therefore, a thorough and logical approach to the diagnosis of abdominal pain is necessary.
|
Pain location | Possible diagnoses | |
Right upper quadrant | Biliary: cholecystitis, cholelithiasis, cholangitis
Colonic: colitis, diverticulitis
Hepatic: abscess, hepatitis, ma
Pulmonary: pneumonia, embolu
Renal: nephrolithiasis, pyelonephritis | |
Epigastric | Biliary: cholecystitis, cholelithiasis, cholang
Cardiac: myocardial infarction, pericarditis
Gastric: esophagitis, gastritis, peptic ulcer
Pancreatic: mass, pancreatitis
Vascular: aortic dissection, mesenteric ischemia | |
Left upper quadrant | Cardiac: angina, myocardial infarction, pericarditis
Gastric: esophagitis, gastritis, peptic ulcer
Pancreatic: mass, pancreatitis
Renal: nephrolithiasis, pyelonephritis
Vascular: aortic dissection, mesenteric ischemia | |
Periumbilical | Colonic: early appendicitis
Gastric: esophagitis, gastritis, peptic ulcer, small-bowel mass or obstruction
Vascular: aortic dissection, mesenteric ischemia | |
Right lower quadrant | Colonic: appendicitis, colitis, diverticulitis, IBD, IBS
Gynecologic: ectopic pregnancy, fibroids, ovarian mass, torsion, PID
Renal: nephrolithiasis, pyelonephritis | |
Suprapubic | Colonic: appendicitis, colitis, diverticulitis, IBD, IBS
Gynecologic: ectopic pregnancy, fibroids, ovarian mass, torsion, PID
Renal: cystitis, nephrolithiasis, pyelonephritis | |
Left lower quadrant | Colonic: colitis, diverticulitis, IBD, IBS
Gynecologic: ectopic pregnancy, fibroids, ovarian mass, torsion, PID
Renal: nephrolithiasis, pyelonephritis | |
Any location | Abdominal wall: herpes zoster, muscle strain, hernia
Other: bowel obstruction, mesenteric ischemia, peritonitis, narcotic withdrawal, sickle cell crisis, porphyria, IBD, heavy metal poisoning
|
Thoracic surgery emergencies
What are examples of life threatening thoracic conditions?
Airway obstruction
Tension pneumothorax
Massive haemothorax
Open pneumothorax
Flail chest segment with pulmonary contusion
Cardiac tamponade.
|
Colon and rectal surgery emergencies
Injury to the Colon and Rectum (stab wound)
Hemorrhoids
Fissures (painful tears in the anal lining)
Abscesses and fistulaes (infections located around the anus and rectum).
Hemorrhage of rectum and anus
How should you manage a stab wound that caused prolapse of intestines?
Do not do any laparotomy.
Do not cut any site or location in this situation.
Relocate the intestines to original location and suture the stab wound.
Critical monitoring of the individual is required.
Make a police report of the case with punishments of criminals who inflicted stab wound with all other criminal conspirators.
How many of you have come across a case of stab wound with prolapse of intestines?
Where have you reported such cases up to now?
| |
|
Obstetrics emergencies
6 Pregnancy Warning Signs
Vaginal Bleeding
Baby’s Activity Level Significantly Declines
Contractions Early in the Third Trimester
Leakage of Fluid from the Vagina
Headache
Severe Nausea and Vomiting
A Persistent Severe Headache, Abdominal Pain, Visual Disturbances, and Swelling During Your Third Trimester
The first principles of dealing with obstetric emergencies are the same as for any emergency (see to the airway, breathing, and circulation), but remember that in obstetrics there are two patients; the fetus is very vulnerable to maternal hypoxia
Abruption of the placenta
Placenta praevia
Postpartum haemorrhage
Amniotic fluid embolism
Inversion of uterus
Infection
Psychological conditions
Stillbirth and intrauterine death
Clinical features of abruption of the placenta
Symptoms
•Abdominal pain
•Severe shock with symptoms beyond vaginal blood loss
•Vaginal bleeding—usually old blood
Signs
•Shock
•Spasm of uterus—described as woody
•Tender uterus
•Fetal parts hard to feel
•Often no fetal heart is heard
All emergency protocols should have been considered beforehand and mutually agreed by obstetricians, midwives, general practitioners, and paramedics. Everybody then knows their immediate priority, and hazards to the woman can be minimised.
Abruption of the placenta
An abruption is a death threat to the fetus and a hazard to the mother. When the placenta separates from its bed (probably because of the rupture of a malformed blood vessel), the damage to the fetus follows not just because of the barrier that the clot makes between the placental bed and villi but also because the release of prostaglandins causes a major degree of uterine spasm. This interferes with perfusion of the placenta, which remains attached. Blood tracking into the myometrium often goes as far as the peritoneum over the uterus, causing much pain and shock, with spasm of the uterine muscle.
Emergency treatment of abruption
Treat the shock
•Give oxygen
•Insert intravenous lines
•Arrange a cross match of 6 units of blood
•Give morphine (if fetus dead)
Deliver the fetus
•By caesarean section (if fetus is alive and gestation is mature)
•By rupturing membranes (if cervix is ripe or fetus is dead)
Treat disseminated intravascular coagulopathy
•Urgent haematological consultation
•Check platelet count
•Give cryoprecipitate (fresh frozen plasma)
•Transfuse with fresh blood if available
In major degrees of placental abruption the woman is shocked well beyond the apparent amount of blood loss and needs urgent transport into hospital. A wide bore intravenous line should be set up and blood sent for cross matching of at least six units of blood. Until this blood arrives, other plasma expanding fluids, such as Haemaccel, should be used.
If the fetus is still alive and gestation sufficiently advanced, caesarean section is the best management. However, if the fetus is dead, conservative management can be pursued provided that the woman does not continue deteriorating—for example, by developing a coagulopathy. Most women with a severe abruption that kills the fetus will go into spontaneous labour soon and have an easy delivery, but caesarean section is occasionally necessary for maternal indications alone. Treatment must be aimed at the shock and at preventing disseminated intravascular coagulopathy.
Usually the placenta is implanted on the anterior wall of the uterus, but sometimes it is posterior when the abruption is less painful and not so severe that the mother is shocked; the fetus may still be at risk, however. Diagnosis in these cases is by recognition of the excessively frequent contractions produced by the prostaglandin release and the abnormal pattern of the fetal heart rate secondary to fetal hypoxia; these are best shown with cardiotocography, a priority investigation in all women admitted with abdominal pain in pregnancy.
Placenta praevia
The blastocyst occasionally implants in the lower part of the uterus. Stretching and thinning of the uterine muscle of the lower segment in the third trimester may sheer off part of the placental attachment. This is accompanied by painless bleeding.
Clinical aspects of placenta praevia
Symptoms
•Vaginal bleeding—bright red, painless, recurrent
Signs
•Soft, pain free uterus
•Easy to feel fetus—often high head, breech, or transverse lie
•No fetal distress
•Do not do a digital vaginal examination
•A speculum examination in an inpatient to exclude any local bleeding is acceptable
Often the fetus is not affected by the first small bleeds, but they should be taken seriously for there is a risk that the mother could have a much larger bleed. Hence, women with bright red, painless vaginal bleeding are considered to have placenta praevia until proved otherwise and should be admitted to hospital. Vaginal ultrasound examination is the best technique for investigating possible placenta praevia, but, although it has a high sensitivity and specificity for central placenta praevia in the third trimester, it is much less precise in the late second trimester or for marginal placenta praevia. Management should therefore always be based on appropriate clinical judgment.
If placenta praevia is confirmed the woman should stay in hospital for at least 48 hours after the bleeding has stopped. Management is conservative, even to the level of giving blood transfusions for severe bleeds, until the fetus is mature (at about 36 weeks). Studies do not show any benefit in keeping women in hospital until delivery, provided that they have a telephone at home and live close enough to the hospital to be brought in by the emergency services within 20 minutes if they start bleeding again (Love et al, 1996). Unless it is very obvious—for example, a complete placenta praevia on ultrasound examination, together with a transverse lie of the fetus—placenta praevia is sometimes confirmed by examination under general anaesthesia in theatre, proceeding in most instances to caesarean section performed by a senior obstetrician. Occasionally, if the placenta is anterior and only just engaging in the lower segment, the membranes may be ruptured and a vaginal delivery expected, as the head coming down into the mother’s pelvis will compress the bleeding placental bed against the back of the pubis symphysis. The same cannot be said for any degree of posterior placenta praevia.
After delivery, a postpartum haemorrhage is likely because the placental bed is situated over less well contracting uterine muscle and may well bleed despite oxytocic stimulation. This often requires blood transfusion.
Postpartum haemorrhage
After a normal delivery a woman commonly loses up to 300 ml of blood. As her blood volume has increased because of fluid retention during pregnancy, this is a loss which can be coped with readily. However, a loss of >500?ml measured clinically in the first 24 hours is considered to be a primary postpartum haemorrhage. Blood loss is commonly underestimated by the attending practitioners. The mother should be watched carefully and treatments given to prevent any further loss.
Management of primary postpartum haemorrhage
Preventive
•Intramuscular oxytocin at the end of the second stage of labour
Curative
•Repeat oxytocic administration
•Rub up a contraction
•Check completeness of the placenta—if it is not delivered or a lobule is missing, prepare for manual removal
•Bimanual compression
•Intramyometrial prostaglandin E2 or carboprost
•Surgical ligation—uterine arteries, internal iliac arteries, or braces (or Lynch) suture of uterus
•Hysterectomy
If the uterus has not contracted firmly, manual stimulation may work by rubbing up a contraction, and a further oxytocic is given. If the placenta is incomplete the uterine cavity is explored for the remaining lobules whose presence in the uterine cavity may prevent the organ contracting down. If neither of these conditions exists, trauma to the lower uterus, cervix, or upper vagina may be the cause of the bleeding. Such traumas should be looked for (in theatre with a good light) and sutured appropriately. A rare cause of continuing primary postpartum haemorrhage is a rupture of the uterus. This needs diagnosis and treatment with either hysterectomy or abdominal resuturing.
After the first 24 hours, any bleeding is a secondary postpartum haemorrhage. It is commonly associated with infection, which should be treated vigorously with intravenous antibiotics. If it persists, suction evacuation of the uterus should be undertaken by a senior obstetrician; perforation of the soft uterus is a major risk in this situation.
A complication of severe and prolonged blood loss is a consumptive coagulopathy, when the mother’s blood does not clot owing to interference with the clotting cascade. The continuing cooperation of a senior haematologist is essential. The mother continues to bleed not just from the placental bed but from other sites in the body. This needs firm and prompt correction so that full coagulation can be restored. Giving cryoprecipitate (frozen precipitate) provides the missing components.
Amniotic fluid embolism
Occasionally, when the uterus is contracting strongly and there is an opening between the amniotic sac and the uterine veins, a bolus of amniotic fluid is pumped into the circulation. This passes through the heart, and an accumulation of amniotic cells becomes trapped in the pulmonary circulation. The amniotic fluid may cause local disseminated intravascular coagulation, which may spread. This rare condition can occur late in the last trimester or during labour.
Amniotic fluid embolism used to be diagnosed on histology only after a postmortem examination but is now sometimes diagnosed before death. The symptoms include collapse while having strong contractions, shock without any blood loss, sudden dyspnoea, and the production of frothy sputum. Treatment is supportive, with steroids, intravenous plasma expansion, and urgent delivery. This obstetric emergency is rare and has a bad prognosis for both mother and fetus, usually owing to delay in diagnosis.
Inversion of uterus
Very rarely, if misapplied pressure has been used on the uterine fundus or traction on the cord of a non-separated placenta in a multiparous woman, the uterus can dimple and invert. This is a very shocking event as the fundus turns inside out and goes through the cervix into the vagina. Treatment requires an experienced obstetrician, who will try to return the uterus under general anaesthesia. This can be very difficult.
Infection
After delivery the genital tract has several sites of potential ingress of bacteria. The placental bed itself is a large raw area, and ascending infection from the lower genital tract may be assisted by previous intrauterine procedures—for example, forceps delivery. Infection of the cervix or, uncommonly, of the episiotomy site, may also occur; the breast can also be a site of infection in the puerperium.
Treating infections
•Infections manifest themselves by local inflammation (swelling and tenderness) and a raised temperature
•Treatment is local heat to the area, analgesia, and broad spectrum antibiotics until the results of bacteriological swabs are available
•Co-amoxiclav and erythromycin are both good choices because they deal with penicillinase-producing staphylococci and streptococci, especially group B
•Metronidazole is often added for uterine infections
•If the infection persists, anaemia may follow, which may ultimately require a blood transfusion
Psychological conditions
Pregnancy and childbirth are times of high psychological stimulation. Any pre-existing psychological disorder may be exaggerated at this time and requires treatment. Many women go through mood swings (blues) in relation to childbirth, which can usually be managed by sympathetic support. If postnatal depression persists for a week or so, mild antidepressants may be needed, and the Edinburgh postnatal depression questionnaire may be helpful in diagnosing the condition. If the condition continues, formal psychiatric help is needed.
Three levels of psychiatric state associated with childbirth
Postpartum blues (1 in 5 mothers)
•Transient and treatable by reassurance
Puerpural depression (1 in 10 mothers)
•Low mood, lack of energy, guilt, irritability, and insomnia
•Treated by counselling (midwives and health visitors)
•Antidepressants—refer to GP if depression continues
Puerpural psychosis (1 in 500 mothers)
•Affective, depressive, or manic behaviour; insomnia; confusion; perplexity
•Refer to psychiatrist and admit to mother and baby unit
At the extreme of the spectrum of disease a puerperal psychosis may occur; both the mother and her baby should be admitted to a dedicated maternity/psychiatric unit as both are at risk. Here the mother can have expert psychiatric nursing and medical care while looking after her own baby. There is a 25% risk of recurrence in a future pregnancy.
Stillbirth and intrauterine death
In _______ 3-4 babies per 1000 are stillborn and another 3-4 per 1000 die in the first week of life. The grief reactions in both the woman and her partner need careful management by the midwifery and medical staff. The couple may go through a phase of anger; all hospital and community staff should be trained to cope with this. Midwifery and medical staff must be prepared to listen and offer their sympathies without attributing blame.
Parents should be encouraged to agree to a postmortem examination of the fetus and placenta by a skilled paediatric pathologist. Getting permission for this from the couple requires sensitivity. If a full postmortem examination is declined, a limited examination of the baby may be acceptable (x ray examination, computed tomography, blood samples from the heart area for chromosome analysis, and bacteriological swabbing of the relevant areas of the body).
Cultural attitudes of the parents influence these decisions and must be respected. It is probable that the couple will not object to full histological examination of the placenta.
Here are further guidelines.
|
Gynecologic surgery emergencies
Adnexal torsion
Tubo-ovarian abscess, hemorrhagic ovarian cysts
Gynecologic hemorrhage
Vulvovaginal trauma. |
Neurosurgical Emergencies
Neurological surgery emergencies
Subarachnoid hemorrhage
Intracranial Hemorrhage
Brain AVM (arteriovenous malformation)
Spine Fracture
CaudaEquina
Penetrating Injury
Intracranial Lesions –Focal
Open Skull fracture
Head Trauma
Cushing response
Epidural Hematomas
Epidural Hemorrhage
Uncal Herniation
Pituitary Adenoma
Pituitary apoplexy
Traumatic Compression Fracture
Jumped facets
Ballistic trauma or gunshot wound (GSW)
Shunt malfunction
T7-8 corptectomyand T6-T9 fusion
Cord compression
Clinical signs of high ICP
Here are further guidelines.
|
New Surgical Technique
General surgery
| |
Orthopaedic surgery
| |
Urology
| |
Neurosurgery
| |
Plastic Surgery
|
Surgical Skills
Do you know various surgical skills?
What are various surgical skills?
What is a surgical technique?
A systematic surgical procedure by which a medical condition is treated.
What questions should you answer in case you introduce new surgical technique?
Is this a new surgical technique or already listed in surgical skills practiced by others on human beings?
New Surgical Technique
Is there any specific name for this new surgical technique?
What is the name of this new surgical technique?
Have you discussed with other doctors the benefits, complications, and harms due to this new surgical technique?
For what type of patients is diagnosis and treatment with this new surgical technique useful?
How is this surgical technique going to improve the condition of the patient?
How is this surgical technique performed, from beginning to end?
For what medical condition is this surgical technique the only option of treatment?
What issues is this medical condition causing the patient?
What complications can occur due to this surgical technique?
|
Orthopaedic surgery emergencies
Top 10 pediatric orthopaedic surgical emergencies: a case-based approach for the surgeon on call.
Pediatric patients who require orthopaedic surgical emergency care are often treated by orthopaedic surgeons who primarily treat adult patients. Essential information is needed to safely evaluate and treat the most common surgical emergencies in pediatric patients, including hip fractures; supracondylar humeral, femoral, and tibial conditions of the hip (such as slipped capital femoral epiphysis and septic arthritis); and limb- and life-threatening pathologies, including compartment syndrome, the dysvascular limb, cervical spine trauma, and the polytraumatized child.
Open fractures (bone is exposed outside of a wound)
Open Fractures or Joints
Fractures with joint involvement
Isolated breaks
Stress fractures
Multiple fractures
Non-union fractures (fractures that do not heal)
Malunion fractures (fractures that heal incorrectly)
Acute Compartment Syndrome
Neurovascular injuries
Joint dislocations
Ligament sprains
Muscle strains
Tendon injuries
Septic Joints
Cauda Equina Syndrome
Here are further guidelines.
|
Fractures
Open Fractures
|
Annotation of definition
| |
|
Cause | |
|
Symptoms | |
|
Diagnosis and Treatment | |
|
Description | |
|
Doctor Examination and Initial Treatment | |
|
Gustilo Classification for Open Fractures | |
|
Treatment | |
|
Complications | |
|
Osteology | |
|
Skeletal System
| |
|
Recovery | |
|
Prevention | |
|
Research
|
What are Fractures?
A fracture is the medical term for a broken bone.
What are common types of fractures?
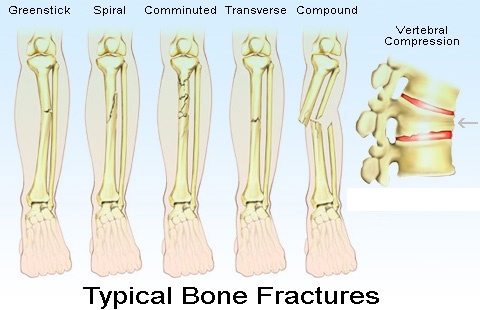


Some fracture types are:
• A Greenstick fracture is an incomplete fracture in which the bone is bent. This type occurs most often in children.
• A transverse fracture is when the broken piece of bone is at a right angle to the bone's axis.
• An oblique fracture is when the break has a curved or sloped pattern.
• A comminuted fracture is when the bone breaks into several pieces.
• A buckled fracture, also known as an impacted fracture, is one whose ends are driven into each other. This is commonly seen in arm fractures in children.
• A pathologic fracture is caused by a disease that weakens the bones.
• A stress fracture is a hairline crack.
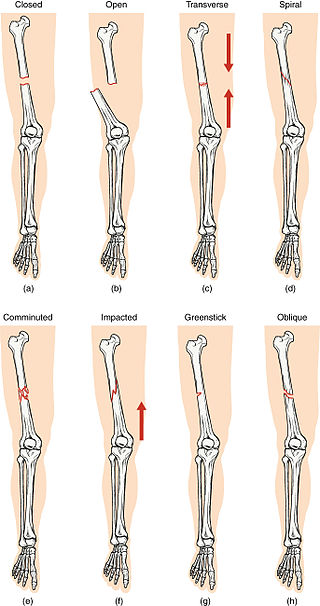
Compare healthy bone with different types of fractures:
(a) closed fracture
(b) open fracture
(c) transverse fracture
(d) spiral fracture
(e) comminuted fracture
(f) impacted fracture
(g) greenstick fracture
(h) oblique fracture
What are the most common types of fractures?
The most common types of fractures in older adults are fractures to the pelvis, hip, femur, vertebrae, humerus, hand, forearm, leg, and ankle.
What is an open (compound) fracture?
An open (or compound) fracture occurs when the skin overlying a fracture is broken, allowing communication between the fracture and the external environment.
What is Human Anatomy?
How will study of this subject help in diagnosis of human medical conditions, medical advice as per international standards and recent advances, as per preventive and curative concepts of medicine?
Let's examine this question.
Which splints and casts should be used for various injuries?
What bones, muscles, arteries, veins, nerves, are associated with this injury or fracture?
Which structures and movements are affected with this injury or fracture?
What will happen if you don't immediately manage an injury or fracture?
Where and when will you use a nail, screw, rod, plate in fixation of a fracture?
This is an orthopedics question. To answer this question correctly.
You have to know about human bones, muscles, arteries, veins, nerves and all related subjects.
What are the most common fractures?
How many total fracture cases were reported every year from last 20 years?
What are the most common fractures reported at your hospital every year?
How many reported fractures were operated?
How many developed post operative deformities?
Do you know anyone who developed post operative deformity?
Did you developer any post operative deformity?
Bones
How many bones are in the human body?
What is the longest bone in the human body?
What is the smallest bone in the human body?
What are the bones of upper limb?
What are the bones of lower limb?
What comes under axial skeleton?
What muscles originate from each bone?
What are the main foramen of base of skull?
What structures pass through each foramen?
How do bones form?
How do bones grow?
What types of cells form bone?
What is the structure of bone?
What materials make up bone?
How do muscles attach to bones?
What is the function of bone?
What are the differences between a human skeleton and a chimpanzee skeleton?
Why do teeth come in different shapes?
How long does it take a bone to heal normally after a fracture?
What is the difference between a splint and a cast?
Which splints and casts should be used for various injuries?
How each is applied?
What should be proper position of the injured extremity?
Why is this the proper position of the injured extremity?
Muscles of upper limb
What are the muscles that move the glenohumeral joint?
What is axial skeleton?
What are the muscles originating on axial skeleton?
What are the muscles originating on scapula?
What are the muscles that move the scapula?
How can the deltoid muscle both extend and flex the arm?
What are the arm muscles that move the elbow joint or forearm?
What are the types of movement?
What are the hand muscles?
What is the origin, insertion, nerve supply and type of movement?
What movements are associated with this muscle?
How does exercise help build muscles?
Cranial nerves
How many total cranial nerves are there?
What is the location of the nucleus of cranial nerves?
What is the pathway from the nucleus to the nerve supply?
How many spinal nerves are there?
Blood
What are the constituents of human blood?
What is hematopoiesis?
Where are hematopoietic stem cells located?
What are the different types and functions of blood cells?
Why and how does total cell count increase during infection?
Here are further guidelines.
Cause
The most common causes of fractures are:
• Trauma. A fall, a motor vehicle accident, or a tackle during a football game can all result in fractures.
• Osteoporosis. This disorder weakens bones and makes them more likely to break.
• Overuse. Repetitive motion can tire muscles and place more force on bone. This can result in stress fractures. Stress fractures are more common in athletes.
Symptoms
Many fractures are very painful and may prevent you from moving the injured area. Other common symptoms include:
•Swelling and tenderness around the injury
•Bruising
•Deformity — a limb may look "out of place" or a part of the bone may puncture through the skin
Doctor Examination
Your doctor will do a careful examination to assess your overall condition, as well as the extent of the injury. He or she will talk with you about how the injury occurred, your symptoms, and medical history.
The most common way to evaluate a fracture is with x-rays, which provide clear images of bone. Your doctor will likely use an x-ray to verify the diagnosis. X-rays can show whether a bone is intact or broken. They can also show the type of fracture and exactly where it is located within the bone.
Treatment
Medication
Splint
Cast (or brace)
Traction
Internal fixation - implantation of plates, screws, pins and rods to set bones and facilitate healing
External fixation – pins, screws and rods placed outside the body to set bones and facilitate healing. External fixators are sometimes used prior to surgical treatment.
Surgery, including minimally invasive surgery performed through small incisions
Bone stimulator (non-surgical) and bone grafting (surgical) for non-union fractures
Evaluation of non-union fractures to identify why a bone did not heal correctly. For example factors such as diabetes, smoking or a thyroid condition may affect a bone’s ability to heal.
Splint
Commonly used splints
Sugar Tong - Used for the forearm or wrist. They are named "sugar-tong" due to their long, U-shaped characteristics, similar to a type of utensil used to pick up sugar cubes
Ulnar Gutter - Used for the forearm to the palm
Volar Wrist Splint - Used for the wrist
Thumb Spica - Used for the thumb
Posterior Lower Leg
Posterior Full Leg
Posterior Elbow
Finger Splints - Used for the fingers
Ankle Stirrup - Used for the ankles
Wrist/arm splint - Used for the wrist or arm
Nasal splint
Cast (or brace)
Cast Types and Maintenance Instructions
What is a cast?
A cast holds a broken bone in place as it heals. Casts also help to prevent or decrease muscle contractions, and are effective at providing immobilization, especially after surgery.
Casts immobilize the joint above and the joint below the area that is to be kept straight and without motion. For example, a child with a forearm fracture will have a long arm cast to immobilize the wrist and elbow joints.
What are casts made of?
The outside, or hard part of the cast, is made from two different kinds of casting materials.
•Plaster (white in color)
•Fiberglass (comes in a variety of colors, patterns, and designs)
Cotton and other synthetic materials are used to line the inside of the cast to make it soft and to provide padding around bony areas, such as the wrist or elbow.
Special waterproof cast liners may be used under a fiberglass cast, allowing the child to get the cast wet. Consult your child's doctor for special cast care instructions for this type of cast.
What are the different types of casts?
Below is a description of the various types of casts, the location of the body they are applied, and their general function.
Type of cast
Location
Uses
Short arm cast
Long arm cast
Arm cylinder cast
|
Applied below the elbow to the hand. | Forearm or wrist fractures. Also used to hold the forearm or wrist muscles and tendons in place after surgery.
| |
Applied from the upper arm to the hand. | Upper arm, elbow, or forearm fractures. Also used to hold the arm or elbow muscles and tendons in place after surgery.
| |
Applied from the upper arm to the wrist. | To hold the elbow muscles and tendons in place after a dislocation or surgery.
|
Type of cast
Location
Uses
Shoulder spica cast
Minerva cast
Short leg cast
Leg cylinder cast
|
Applied around the trunk of the body to the shoulder, arm, and hand. |
Shoulder dislocations or after surgery on the shoulder area. | |
Applied around the neck and trunk of the body. |
After surgery on the neck or upper back area. | |
Applied to the area below the knee to the foot. |
Lower leg fractures, severe ankle sprains/strains, or fractures. Also used to hold the leg or foot muscles and tendons in place after surgery to allow healing. | |
Applied from the upper thigh to the ankle. |
Knee, or lower leg fractures, knee dislocations, or after surgery on the leg or knee area.
|
Type of cast
Location
Uses
Unilateral hip spica cast
One and one-half hip spica cast
Bilateral long leg hip spica cast
|
Applied from the chest to the foot on one leg. |
Thigh fractures. Also used to hold the hip or thigh muscles and tendons in place after surgery to allow healing.
| |
Applied from the chest to the foot on one leg to the knee of the other leg. A bar is placed between both legs to keep the hips and legs immobilized. |
Thigh fracture. Also used to hold the hip or thigh muscles and tendons in place after surgery to allow healing.
| |
Applied from the chest to the feet. A bar is placed between both legs to keep the hips and legs immobilized. |
Pelvis, hip, or thigh fractures. Also used to hold the hip or thigh muscles and tendons in place after surgery to allow healing.
|
Type of cast
Location
Uses
Short leg hip spica cast
|
Applied from the chest to the thighs or knees. |
To hold the hip muscles and tendons in place after surgery to allow healing.
|

Type of cast
Location
Uses
Abduction boot cast
|
Applied from the upper thighs to the feet. A bar is placed between both legs to keep the hips and legs immobilized.
|
To hold the hip muscles and tendons in place after surgery to allow healing.
|
How can your child move around while in a cast?
Assistive devices for children with casts include:
•Crutches
•Walkers
•Wagons
•Wheelchairs
•Reclining wheelchairs
Cast care instructions
•Keep the cast clean and dry.
•Check for cracks or breaks in the cast.
•Rough edges can be padded to protect the skin from scratches.
•Do not scratch the skin under the cast by inserting objects inside the cast.
•Can use a hairdryer placed on a cool setting to blow air under the cast and cool down the hot, itchy skin. Never blow warm or hot air into the cast.
•Do not put powders or lotion inside the cast.
•Cover the cast while your child is eating to prevent food spills and crumbs from entering the cast.
•Prevent small toys or objects from being put inside the cast.
•Elevate the cast above the level of the heart to decrease swelling.
•Encourage your child to move his or her fingers or toes to promote circulation.
•Do not use the abduction bar on the cast to lift or carry the child.
Older children with body casts may need to use a bedpan or urinal in order to go to the bathroom. Tips to keep body casts clean and dry and prevent skin irritation around the genital area include the following:
•Use a diaper or sanitary napkin around the genital area to prevent leakage or splashing of urine.
•Place toilet paper inside the bedpan to prevent urine from splashing onto the cast or bed.
•Keep the genital area as clean and dry as possible to prevent skin irritation.
When to call your child's doctor
Contact your child's doctor or healthcare provider if your child develops one or more of the following symptoms:
•Fever as directed by your healthcare provider or:
• Your child is younger than 12 weeks and has a fever of 100.4°F (38°C) or higher because your baby may need to be seen by their healthcare provider.
• Your child has repeated fevers above 104°F (40°C) at any age.
• Your child is younger than 2 years old and their fever continues for more than 24 hours or your child is 2 years old and older and their fever continues for more than 3 day
•Increased pain
•Increased swelling above or below the cast
•Decreased ability to move extremity in the cast
•Complaints of numbness or tingling
•Drainage or foul odor from the cast
•Cool or cold fingers or toes
•If the cast becomes wet or soiled
•Blister, sores, or rash develop under the cast
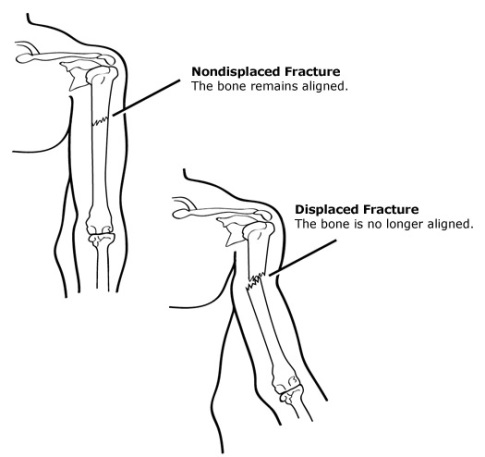
All forms of treatment of broken bones follow one basic rule: the broken pieces must be put back into position and prevented from moving out of place until they are healed. In many cases, the doctor will restore parts of a broken bone back to the original position. The technical term for this process is "reduction."
Broken bone ends heal by "knitting" back together with new bone being formed around the edge of the broken parts.
Surgery is sometimes required to treat a fracture. The type of treatment required depends on the severity of the break, whether it is "open" or "closed," and the specific bone involved. For example, a broken bone in the spine (vertebra) is treated differently from a broken leg bone or a broken hip.
Doctors use a variety of treatments to treat fractures:
About Casts
Casts and splints support and protect injured bones and soft tissue. When you break a bone, your doctor will put the pieces back together in the right position. Casts and splints hold the bones in place while they heal. They also reduce pain, swelling, and muscle spasm.
Splints and casts are sometimes applied after surgery.
What are the different kinds of casts?
A cast, which keeps a bone from moving so it can heal, is essentially a big bandage that has two layers — a soft cotton layer that rests against the skin and a hard outer layer that prevents the broken bone from moving.
These days, casts are made of either:
•plaster of paris: a heavy white powder that forms a thick paste that hardens quickly when mixed with water. Plaster of paris casts are heavier than fiberglass casts and don't hold up well in water.
•synthetic (fiberglass) material: made out of fiberglass, a kind of moldable plastic, these casts come in many bright colors and are lighter. The covering (fiberglass) on synthetic casts is water-resistant, but the padding underneath is not. You can, however, get a waterproof liner. The doctor putting on the cast will decide whether a fiberglass cast with a waterproof lining is appropriate.
Orthopedic cast
Cast types
Upper extremity casts
Lower extremity casts
Cylinder cast
Body casts
EDF cast
Spica cast
Mobility and hygiene
Other casts
Cast-cutting
Removal of Plaster Casts
How is a cast put on?
First, several layers of soft cotton are wrapped around the injured area. Next, the plaster or fiberglass outer layer is soaked in water. The doctor wraps the plaster or fiberglass around the soft first layer. The outer layer is wet but will dry to a hard, protective covering. Doctors sometimes make tiny cuts in the sides of a cast to allow room for swelling.
Can plaster of paris casts get wet?
Absolutely not! A wet cast may not hold the bone in place because the cast could start to dissolve in the water and could irritate the skin underneath it, possibly leading to infection. So your child shouldn't swim and should use a plastic bag or special sleeve (available online or sometimes at pharmacies) to protect the cast from water. And instead of a shower, your child may need to take a sponge bath.
Can synthetic (fiberglass) casts get wet?
Although the fiberglass itself is waterproof, the padding inside a fiberglass cast is not. So it's still important to try to keep a fiberglass cast from getting wet. If this is a problem, talk to the doctor about getting a waterproof liner. Fiberglass casts with waterproof liners let kids continue bathing or even go swimming during the healing process. Although the liner allows for evaporation of water and sweat, it's still fragile. Also, only certain types of breaks can be treated with this type of cast. Your doctor will determine if the fracture may be safely treated with a waterproof cast.
Cast Immobilization
A plaster or fiberglass cast is the most common type of fracture treatment, because most broken bones can heal successfully once they have been repositioned and a cast has been applied to keep the broken ends in proper position while they heal.
Functional Cast or Brace
The cast or brace allows limited or "controlled" movement of nearby joints. This treatment is desirable for some, but not all, fractures.
Traction
Traction is usually used to align a bone or bones by a gentle, steady pulling action.
External Fixation
In this type of operation, metal pins or screws are placed into the broken bone above and below the fracture site. The pins or screws are connected to a metal bar outside the skin. This device is a stabilizing frame that holds the bones in the proper position while they heal.
In cases where the skin and other soft tissues around the fracture are badly damaged, an external fixator may be applied until surgery can be tolerated.
An external fixator applied to a broken thighbone.
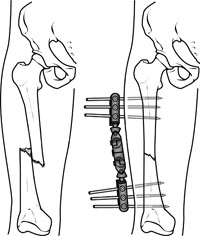
Open Reduction and Internal Fixation
During this operation, the bone fragments are first repositioned (reduced) in their normal alignment, and then held together with special screws or by attaching metal plates to the outer surface of the bone. The fragments may also be held together by inserting rods down through the marrow space in the center of the bone.
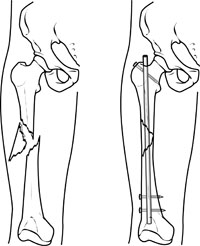
A specially designed metal rod, called an intramedullary nail, provides strong fixation for this thighbone fracture.

The broken bones of the forearm are held in position by plates and screws while they heal.
Recovery
Fractures take several weeks to several months to heal, depending on the extent of the injury and how well you follow your doctor's advice. Pain usually stops long before the fracture is solid enough to handle the stresses of normal activity.
Even after your cast or brace is removed, you may need to continue limiting your movement until the bone is solid enough for normal activity.
During your recovery you will likely lose muscle strength in the injured area. Specific exercises will help you restore normal muscle strength, joint motion, and flexibility.
Prevention
Preventing Falls and Related Fractures
Several factors can lead to a fall. Loss of footing or traction is a common cause of falls. Loss of footing occurs when there is less than total contact between one’s foot and the ground or floor. Loss of traction occurs when one’s feet slip on wet or slippery ground or floor. Other examples of loss of traction include tripping, especially over uneven surfaces such as sidewalks, curbs, or floor elevations that result from carpeting, risers, or scatter rugs. Loss of footing also happens from using household items intended for other purposes – for example, climbing on kitchen chairs or balancing on boxes or books to increase height.
A fall may occur because a person’s reflexes have changed. As people age, reflexes slow down. Reflexes are automatic responses to stimuli in the environment. Examples of reflexes include quickly slamming on the car brakes when a child runs into the street or quickly moving out of the way when something accidentally falls. Aging slows a person’s reaction time and makes it harder to regain one’s balance following a sudden movement or shift of body weight.
Improving Balance
Do muscle-strengthening exercises.
Obtain maximum vision correction.
Practice using bifocal or trifocal glasses.
Practice balance exercises daily.
Changes in muscle mass and body fat also can play a role in falls. As people get older, they lose muscle mass because they have become less active over time. Loss of muscle mass, especially in the legs, reduces one’s strength to the point where she or he is often unable to get up from a chair without assistance. In addition, as people age, they lose body fat that has cushioned and protected bony areas, such as the hips. This loss of cushioning also affects the soles of the feet, which upsets the person’s ability to balance. The gradual loss of muscle strength, which is common in older people but not inevitable, also plays a role in falling. Muscle-strengthening exercises can help people regain their balance, level of activity, and alertness no matter what their age.
Changes in vision also increase the risk of falling. Diminished vision can be corrected with glasses. However, often these glasses are bifocal or trifocal so that when the person looks down through the lower half of her or his glasses, depth perception is altered. This makes it easy to lose one’s balance and fall. To prevent this from happening, people who wear bifocals or trifocals must practice looking straight ahead and lowering their head. For many other older people, vision changes cannot be corrected completely, making even the home environment hazardous.
Safety first to prevent falls: At any age, people can change their environments to reduce their risk of falling and breaking a bone.
Outdoor safety tips:
In nasty weather, use a walker or cane for added stability.
Wear warm boots with rubber soles for added traction.
Look carefully at floor surfaces in public buildings. Many floors are made of highly polished marble or tile that can be very slippery. If floors have plastic or carpet runners in place, stay on them whenever possible.
Identify community services that can provide assistance, such as 24-hour pharmacies and grocery stores that take orders over the phone and deliver. It is especially important to use these services in bad weather.
Use a shoulder bag, fanny pack, or backpack to leave hands free.
Stop at curbs and check their height before stepping up or down. Be cautious at curbs that have been cut away to allow access for bikes or wheelchairs. The incline up or down may lead to a fall.
Indoor safety tips:
Keep all rooms free from clutter, especially the floors.
Keep floor surfaces smooth but not slippery. When entering rooms, be aware of differences in floor levels and thresholds.
Wear supportive, low-heeled shoes, even at home. Avoid walking around in socks, stockings, or floppy, backless slippers.
Check that all carpets and area rugs have skid-proof backing or are tacked to the floor, including carpeting on stairs.
Keep electrical and telephone cords and wires out of walkways.
Be sure that all stairwells are adequately lit and that stairs have handrails on both sides. Consider placing fluorescent tape on the edges of the top and bottom steps.
For optimal safety, install grab bars on bathroom walls beside tubs, showers, and toilets. If you are unstable on your feet, consider using a plastic chair with a back and nonskid leg tips in the shower.
Use a rubber bath mat in the shower or tub.
Keep a flashlight with fresh batteries beside your bed.
Add ceiling fixtures to rooms lit by lamps only, or install lamps that can be turned on by a switch near the entry point into the room. Another option is to install voice- or sound-activated lamps.
Use bright light bulbs in your home.
If you must use a step-stool for hard-to-reach areas, use a sturdy one with a handrail and wide steps. A better option is to reorganize work and storage areas to minimize the need for stooping or excessive reaching.
Consider purchasing a portable phone that you can take with you from room to room. It provides security because you can answer the phone without rushing for it and you can call for help should an accident occur.
Don’t let prescriptions run low. Always keep at least 1 week’s worth of medications on hand at home. Check prescriptions with your doctor and pharmacist to see if they may be increasing your risk of falling. If you take multiple medications, check with your doctor and pharmacist about possible interactions between the different medications.
Arrange with a family member or friend for daily contact. Try to have at least one person who knows where you are.
If you live alone, you may wish to contract with a monitoring company that will respond to your call 24 hours a day.
Watch yourself in a mirror. Does your body lean or sway back and forth or side to side? People with decreased ability to balance often have a high degree of body sway and are more likely to fall.
Medications That May Increase the Risk of Falling
Unfortunately, as you get older, you're more likely to need daily medications. And all medications have side effects, some of which can increase your risk of having a fall. Medications that can cause dizziness or lack of coordination are:
•Sedatives or sleeping pills
•Drugs that lower high blood pressure, which can sometimes cause hypotension, blood pressure that is too low
• Antidepressants
•Anticonvulsants, which are used to treat epilepsy and some psychological conditions
•Muscle relaxants, which may be used for back pain or other problems
•Some medicines for heart conditions
Injury Prevention - Seat Belts
Seat Belts
Lap/shoulder safety belts, when used correctly, reduce the risk of death to front seat occupants by 45% and risk of moderate to critical injury by 50%.
Food and Your Bones
Proper diet and exercise may help in preventing some fractures. A diet rich in calcium and Vitamin D will promote bone strength. Weightbearing exercise also helps keep bones strong.
Getting the calcium and vitamin D you need is easier than you think -- if you eat the right foods.
|
Breakfast Foods | Average Calcium (mg) | |
Cereal, calcium-fortified, 1 cup | 100 - 1000 | |
Soy milk, calcium-fortified, 8 ounces | 80 - 500 | |
Milk (nonfat, 2%, whole, or lactose-reduced), 1 cup | 300 | |
Yogurt, 1 cup | 300 - 400 | |
Orange juice, calcium-fortified | 200 - 340
|
|
Lunch, Dinner, and Snack Foods | Average Calcium (mg) | |
Canned sardines, 3 ounces |
320 | |
Swiss cheese, 1 ounce |
270 | |
Cheddar cheese, 1 ounce |
200 | |
Canned salmon, 3 ounces |
200 | |
Turnip greens, 1 cup |
200 | |
Kale cooked, 1 cup |
90 | |
Broccoli, raw, 1 cup |
90
|
|
What is emergency surgery?
Surgical emergency is a medical emergency which requires immediate surgical intervention (the only way to solve the problem successfully).
How should emergency surgeries be classified?
Extremely urgent emergency surgery
Urgent emergency surgeries
Appendectomy
Setting of a broken bone that needs internal setting
What cases need emergency surgery?
What cases need an emergency operating room (OR)?
The following conditions are surgical emergencies:
Acute trauma
Amputation
Acute appendicitis(Is acute appendicitis a surgical emergency?
Urgent appendectomy has become the basis of management for acute appendicitis because of the disparity in morbidity and mortality rates between perforated and nonperforated appendicitis.)
Abscesses
Aortic dissection
Acute subdural hematoma
Acute airway obstruction
Acute mesenteric ischemia
Bleeding ectopic pregnancy
Bowel obstruction
Cardiac tamponade
Cholecystitis (gallbladder infection)
Diverticulitis
Gastrointestinal perforation
Incarcerated hernia
Intestinal blockage/obstruction
Intestinal volvulus
Internal bleeding
Limb ischemia
Neuroendocrine tumors causing acute homeostatic imbalance unresponsive to medication (often due to decompensation)
Pneumothorax
Paraphimosis
Peritonitis
Ruptured intestine
Ruptured aortic aneurysm
Retinal detachment
Retained abortion
Spleen Removal
Stercoral perforation
Thrombosed hemorrhoids
Testicular torsion
Urinary retention (not respond to other medical treatment)
|
Pediatric surgery emergencies
Congenital
Nontraumatic Pediatric Surgical Emergencies
Pediatric Trauma
Nontraumatic Pediatric Surgical Emergencies
-
Appendicitis
-
Management of epistaxis in children
-
Balanoposthitis in children: Clinical manifestations, diagnosis, and treatment
-
Overview of inguinal hernia in children
-
Incarcerated Inguinal hernia
-
Intestinal malrotation
-
Intussusception in children
-
Infantile hypertrophic pyloric stenosis
-
Rectal prolapse
-
Intussusception
-
Pyloric Stenosis
-
Bowel Obstruction
Atresias
Hirschsprung’s
Malrotation
Volvulus
Intussusception
-
Foreign Bodies
-
Hirschsprung’s Enterocolitis
-
Malrotation with volvulus
What are the important points about the history?
What are the pertinent physical findings?
How is the problem managed?
What is the differential diagnosis?
What further workup is needed?
When/if to do surgery?
Anesthesia for Common Pediatric Surgical Emergencies: Are You Well Equipped?
Postop management
Acute trauma
Pediatric orthopaedic surgical emergencies
-
Hip fractures; supracondylar humeral, femoral, and tibial conditions of the hip (such as slipped capital femoral epiphysis and septic arthritis); and limb- and life-threatening pathologies, including compartment syndrome, the dysvascular limb, cervical spine trauma, and the polytraumatized child.
Adults (age 19 and older)
-
Open Fractures
-
Acute Compartment Syndrome
-
Neurovascular injuries
-
Dislocations
-
Septic Joints
-
Cauda Equina Syndrome
Cardiothoracic
-
Cardiac tamponade
-
Acute airway obstruction
-
Pneumothorax
Gastrointestinal
-
Acute appendicitis
-
Bowel obstruction
-
Gastrointestinal perforation
-
Intestinal volvulus
-
Acute mesenteric ischemia
-
Peritonitis
-
Stercoral perforation
Genitourinary
-
Testicular torsion
-
Urinary retention
-
Paraphimosis
-
Priapism
Gynaecological
-
Bleeding ectopic pregnancy
-
Retained abortion
Neurological/Ophthalmic
-
Acute subdural hematoma
-
Retinal detachment
Vascular
-
Ruptured aortic aneurysm
-
Aortic dissection
-
Internal bleeding
-
Limb ischemia
|
Diagnosis accuracy importance.
Why is diagnosis accuracy essential to any physician surgeon medical emergency, physician surgeon elective surgery?
We will take an example of acute abdominal pain.
There are more than 22 causes of acute abdominal pain.
Acute abdominal pain can represent a spectrum of conditions from benign and self-limited disease to surgical emergencies.
Out of more than 22 causes of acute abdomen, only two causes of acute abdomen need surgical intervention under verified conditions of seniors.
Do not go ahead with surgery without second and third consultation from senior physicians for verification of diagnosis and appropriate treatment.
|
Surgical Skills
Do you know various surgical skills?
What are various surgical skills?
What is a surgical technique?
A systematic surgical procedure by which a medical condition is treated.
Here are further guidelines.
|
Seniority
What should other physicians who claim to be surgeons know?
Physician surgeon medical emergency
Physician surgeon elective surgery
These are the only two types of entities of physicians with surgical abilities.
How should seniority of physician surgeon medical emergency, physician surgeon elective surgery be categorized?
Guide to physician surgeon medical emergency, physician surgeon elective surgery is most senior, for example the individual circulating these guidelines www.qureshiuniversity.com/surgeryworld.html Doctor Asif Qureshi.
You must know Doctor Asif Qureshi guides at least 812 other various professions, for example www.qureshiuniversity.com/professionsworld.html
Do not expect Doctor Asif Qureshi to reach out to your operating room and, for example, in cholecystectomy for gallstones do 8-inch Incision, clamp at two ends of gall bladder, cut, suture the stump, and close in 3 layers. Juniors have to perform these services.
Do not expect Doctor Asif Qureshi to reach out to medical emergency room and, for example, trauma with head injury with scalp laceration that needs closure in 2 layers of two ends of lacerated scalp. Juniors have to perform these services. Doctor Asif Qureshi has done these services while he was a junior physician.
If you do not understand anything from www.qureshiuniversity.com/surgeryworld.html you are encouraged to ask questions.
Consultant physician surgeon medical emergency, physician surgeon elective surgery.
Senior resident physician surgeon medical emergency, physician surgeon elective surgery.
Junior resident physician surgeon medical emergency, physician surgeon elective surgery.
How many subcategories of surgeries are there?
14 subcategories of surgical categories have to be recognized that can be emergency or elective.
What should physician surgeon medical emergency know?
You have to know everything of these entities.
What should physician surgeon elective surgery know?
You have to know everything of these entities.
How are other regions categorizing surgical categories?
In some regions, even anethesiologist is expected to have physician surgeon medical emergency, physician surgeon elective surgery abilities.
Here are various subcategories of surgery in other regions that needs to be updated.
|
Anesthesiology |
The specialty of anesthesia during surgery and pain management. | |
Bariatric Surgery |
The specialty of treating obesity with surgery. | |
Cardiac Surgery |
The specialty of treating heart problems with surgery. | |
Cardiothoracic Surgery |
The specialty of treating heart, lung and other problems in the chest with surgery. | |
Colon & Rectal Surgery |
The specialty of treating problems of the small and large intestine, the rectum and anus with surgery. | |
General Surgery |
The specialty of treating common abdominal problems such as hernias and appendicitis with surgery. | |
Gynecologic Surgery |
The specialty of treating problems with the female reproductive system with surgery. | |
Maxillofacial Surgery |
The specialty of treating problems of the mouth, jaw, neck and facial bones with surgery. | |
Neurosurgery |
The specialty of treating the central nervous system, including the brain and spinal cord, with surgery. | |
Obstetrics |
The specialty of treating women before, during and after childbirth which may include surgery such as a C-section. | |
Oncology |
The specialty of treating cancer with surgery. | |
Ophthalmology |
The specialty of treating conditions of the eye with surgery. | |
Oral Surgery |
The specialty of treating dental problems with surgery, such as wisdom tooth removal and root canals. | |
Orthopedic Surgery |
The specialty of treating problems of the bones, joints, ligaments and tendons with surgery. | |
Otolaryngology (Ear, Nose and Throat, ENT ) |
The specialty of treating problems of the ears, nose and throat with surgery. | |
Pediatric Surgery |
The specialty of treating health problems of children with surgery. | |
Plastic Surgery: Cosmetic & Reconstructive Surgery |
The specialty of improving the appearance for cosmetic reasons, or to correct defects for a more appealing appearance.
| |
Podiatry Surgery (Podiatry) |
The specialty of treating problems of the feet with surgery. | |
Thoracic Surgery |
The specialty of treating problems in the chest cavity, except the heart, with surgery. | |
Transplant Surgery |
The specialty of replacing failing organs with donated organs with surgery. | |
Trauma Surgery |
The specialty of treating injuries from car crashes, gunshot wounds, stabbings and other traumatic injuries with surgery.
| |
Vascular Surgery |
The specialty of treating problems of the blood vessels with surgery.
|
Critical, emergency, urgent surgeries have to be performed by physician surgeon medical emergency.
|
|
